Loose bowels in the elderly are more than just an occasional inconvenience. They can signal underlying health issues and significantly impact daily life. Unlike common belief, frequent watery stools or fecal leakage are not normal parts of aging. Instead, they may point to infections, medication side effects, chronic conditions like irritable bowel syndrome, or malabsorption disorders. Left unmanaged, loose bowels can lead to dehydration, electrolyte imbalances, skin breakdown, and even falls due to urgency.
The good news is that most cases can be improved with targeted strategies. This guide provides a clear, actionable roadmap for managing and stopping loose bowels in older adults. You will learn how to identify causes, implement safe home remedies, recognize red flags, and work with healthcare providers for lasting relief.
Identify the Type of Diarrhea

Knowing the specific type of diarrhea helps determine the right treatment. Not all loose stools are the same. Each type has distinct triggers and requires different management.
Recognize Watery Diarrhea
Watery diarrhea involves frequent, large-volume, non-bloody stools. It falls into two subtypes.
Osmotic diarrhea is caused by undigested substances pulling water into the bowel. Common triggers include artificial sweeteners like sorbitol and xylitol, and lactose in dairy. Symptoms stop when fasting.
Secretory diarrhea occurs when fluid is actively secreted into the gut, continuing even during fasting. Causes include C. difficile infection, bile acid malabsorption, or certain medications.
Visual clue: Stools remain liquid throughout the toilet bowl and lack blood or fat.
Spot Fatty Stools (Steatorrhea)
Fatty diarrhea indicates poor fat absorption. Look for these signs.
Bulky, foul-smelling stools that float in the toilet water are key indicators. You may also notice an oily residue in the toilet water after flushing.
This type often stems from pancreatic insufficiency, celiac disease, or small intestinal bacterial overgrowth. It may come with weight loss, bloating after meals, and nutrient deficiencies.
Detect Inflammatory Diarrhea
Inflammatory diarrhea results from intestinal damage or infection. Key signs include small, frequent stools, blood, pus, or mucus in stool, and cramping, fever, or unintentional weight loss.
Conditions like Crohn’s disease, ulcerative colitis, colorectal cancer, or ischemic colitis can cause this. A subtype called microscopic colitis causes chronic watery diarrhea, often at night, and is diagnosed only through colon biopsy.
Rule Out Serious Underlying Conditions
Persistent loose bowels may reflect a deeper medical issue. Early detection improves outcomes and prevents complications.
Check for Infections
Infections are a leading cause of acute diarrhea in seniors. Clostridioides difficile is especially common after antibiotic use or hospital stays. Symptoms include watery diarrhea, abdominal pain, and sometimes fever.
Other pathogens like Salmonella, E. coli, or parasites may be contracted through contaminated food or water. If diarrhea follows travel or recent antibiotics, testing for these should be a priority.
Evaluate for Chronic Diseases
Several long-term conditions mimic or cause loose bowels.
Irritable bowel syndrome with diarrhea is diagnosed after ruling out other causes. It features alternating bowel habits and abdominal discomfort.
Celiac disease is triggered by gluten and may present with diarrhea, anemia, or osteoporosis in older adults.
Pancreatic insufficiency leads to steatorrhea and is treated with enzyme supplements.
Diabetes can cause diabetic neuropathy, which disrupts gut motility and causes erratic bowel movements.
Hyperthyroidism speeds up digestion, resulting in frequent stools.
Blood tests and imaging help confirm or rule out these conditions.
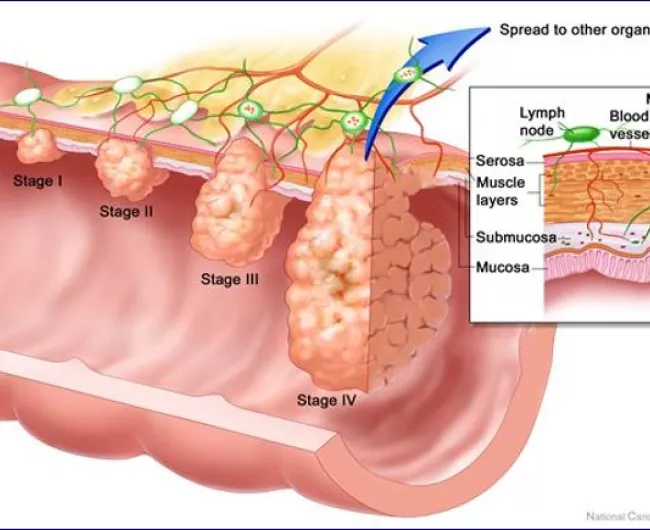
Consider Cancer and Ischemia
Colorectal cancer can cause partial blockage, leading to mucus, bleeding, or changes in bowel habits. Ischemic colitis due to reduced blood flow to the colon is more common in those with heart disease and presents with sudden left-sided abdominal pain and bloody stools.
Both require prompt evaluation, especially if symptoms are new or worsening.
Review Medications That Cause Diarrhea
Polypharmacy is a major but often overlooked cause of loose bowels in seniors. Many commonly prescribed drugs disrupt digestion.
Common Offending Medications
Check for these diarrhea-inducing drugs.
Antibiotics wipe out healthy gut bacteria and increase C. difficile risk.
Proton pump inhibitors reduce stomach acid and raise infection and microscopic colitis risk.
Metformin causes up to 20% of users to experience diarrhea. Switching formulations or medications may help.
Nonsteroidal anti-inflammatory drugs can irritate the gut lining and cause ulcers or colitis.
Magnesium supplements or antacids have an osmotic effect, drawing water into the bowel.
Selective serotonin reuptake inhibitors may alter serotonin levels in the gut and affect motility.
Laxative overuse can lead to dependency and rebound diarrhea.
How to Address Drug-Induced Diarrhea
Work with a doctor or pharmacist to identify potential culprits, adjust dosages, switch to alternatives, or discontinue unnecessary medications.
Never stop prescription drugs without medical guidance.
Implement Immediate Home Care Strategies
For mild, short-term episodes, effective home care can stop loose bowels quickly and safely.
Rehydrate Effectively
Dehydration is the top risk in elderly patients with diarrhea. Replace fluids and electrolytes promptly.
Best options include oral rehydration solutions like Pedialyte or DripDrop, nonfat broth, diluted fruit juice with no pulp, and herbal teas like ginger or chamomile.
Avoid plain water alone, caffeine, alcohol, and carbonated drinks.
Fluid goal is at least 8 to 10 cups, or 64 to 80 ounces, daily, plus 1 extra cup per loose stool.
Watch for signs of dehydration: dry mouth, dizziness, low urine output, and confusion.
Follow a Short-Term Bland Diet
Switch to easily digestible foods to rest the gut.
Use the BRAT diet for 24 to 48 hours only. This includes bananas rich in potassium and pectin, white rice low in fiber, applesauce containing binding pectin, and plain white toast.
This diet lacks protein and nutrients. Do not extend beyond two days.
Add these safe foods: boiled potatoes without skin, saltine crackers, plain oatmeal, cooked carrots, lean chicken or turkey, and noodles without sauce.
Avoid Diarrhea Triggers
Eliminate these during active symptoms: dairy if lactose intolerant, high-fat or fried foods, spicy dishes, raw fruits and vegetables except bananas and applesauce, artificial sweeteners found in sugar-free gum and mints, and caffeine and alcohol.
Restore Gut Health with Probiotics
Rebalancing gut bacteria can shorten diarrhea duration and prevent recurrence.
Choose Effective Strains
Not all probiotics are equal. Look for Lactobacillus rhamnosus GG, Saccharomyces boulardii, or Bifidobacterium species.
These strains have strong evidence for treating antibiotic-associated and infectious diarrhea.
Sources of Probiotics
Probiotics are found in foods like yogurt with live cultures, kefir, sauerkraut, and kimchi. They are also available as supplements in capsule or powder form.
Consult a doctor before starting supplements.
Probiotics work best when combined with prebiotic fiber like bananas and oats to feed beneficial bacteria.
Use OTC Medications Cautiously
Over-the-counter remedies can offer temporary relief, but misuse can be dangerous in older adults.
When to Use Loperamide
Loperamide slows gut movement and allows more water absorption. Use only if there is no fever, no blood in stool, and no known infection.
Dose carefully: Start with 2 milligrams after first loose stool, then 1 milligram after each subsequent one. Maximum is 8 milligrams per day. Avoid long-term use.
Warning: Do not use if infection is suspected. Slowing the gut can trap toxins and cause toxic megacolon.
Consider Bismuth Subsalicylate
Bismuth subsalicylate helps reduce inflammation, kill certain bacteria, and balance fluids.
Benefits include shortening infectious diarrhea and soothing stomach upset.
Risks include turning stool and tongue black, which is harmless. Avoid if on blood thinners or aspirin-sensitive.
Follow label instructions and do not exceed 8 tablets in 24 hours.
Address Fecal Incontinence and Muscle Weakness
Loose bowels often overlap with fecal incontinence, especially in frail or immobile seniors.
Perform Kegel Exercises Daily
Kegels strengthen pelvic floor and anal sphincter muscles.
How to do them: Squeeze muscles used to stop urination or hold in gas. Hold for 3 to 5 seconds. Relax fully. Repeat 10 to 15 times. Do 3 sets per day.
Consistency is key. Improvement takes 4 to 6 weeks.
A pelvic floor physical therapist can guide proper technique and boost results.
Improve Bathroom Access
Mobility issues increase incontinence risk. Ensure a clear, well-lit path to the bathroom. Install grab bars and raised toilet seats. Keep a commode nearby if needed. Dress in loose, easy-to-remove clothing.
Nighttime urgency raises fall risk. Use nightlights and consider scheduled toileting before bed.
Transition to Long-Term Bowel Health
Once acute symptoms resolve, focus on preventing recurrence and supporting digestive stability.
Gradually Increase Fiber Intake
A Harvard study found that women eating 25 grams of fiber daily had an 18% lower risk of fecal incontinence than those consuming only 13.5 grams.
High-fiber foods include legumes like black beans providing 17 grams per cup, whole grains, fruits with skin, and vegetables.
Introduce slowly with plenty of fluids to avoid gas or bloating.
Consider Fiber Supplements
If dietary fiber is insufficient, try psyllium which absorbs water and firms stool, methylcellulose which is gentle and less gas-producing, or partially hydrolyzed guar gum which is well-tolerated and supports gut bacteria.
Mix with water and drink immediately.
Try a Low-FODMAP Diet With Guidance
FODMAPs are fermentable carbs that trigger bloating and diarrhea in sensitive individuals. A low-FODMAP diet can help identify food intolerances.
Common triggers include onions, garlic, beans, lentils, apples, pears, dairy containing lactose, and wheat containing fructans.
Follow this diet under a dietitian’s supervision to avoid nutritional gaps.
Know When to Seek Medical Help
Some symptoms demand immediate evaluation. Do not wait if you notice diarrhea lasting more than 2 to 3 days, signs of dehydration like dizziness, confusion, or dark urine, fever over 101.3 degrees Fahrenheit, blood or mucus in stool, severe abdominal or rectal pain, persistent vomiting, unintentional weight loss, or fecal incontinence disrupting daily life.
In older adults, even mild dehydration can spiral into delirium, falls, or kidney injury.
Diagnostic Tests Your Doctor May Order
If diarrhea persists beyond 72 hours, expect a thorough workup.
Lab and stool testing may include complete blood count and electrolytes to check for infection and dehydration, thyroid panel to rule out hyperthyroidism, celiac blood test, and stool tests for C. difficile, parasites, fecal calprotectin for inflammation, and fat content.
Imaging and endoscopy may include colonoscopy to check for inflammatory bowel disease, cancer, or microscopic colitis, and abdominal CT or ultrasound if structural issues are suspected.
Functional assessments may include anal manometry to measure sphincter pressure and anorectal ultrasound to evaluate muscle integrity.
Explore Advanced Treatments
When conservative methods fail, specialized therapies can restore control.
Try Bile Acid Binders
If bile acid malabsorption is suspected, a trial of cholestyramine, colesevelam, or colestipol may help. Diagnosis can be confirmed with a SeHCAT scan or therapeutic response.
Consider Sacral Nerve Stimulation
Also called a bowel pacemaker, sacral nerve stimulation sends mild electrical pulses to nerves controlling the rectum.
It is most effective for solid stool incontinence and requires surgical implantation. Up to 80% improvement has been seen in controlled studies.
The patient must be able to manage device settings.
This option is ideal for mobile, cognitively intact seniors who have failed other treatments.
Discuss Colostomy as Last Resort
For severe, unmanageable incontinence, a colostomy diverting stool to an abdominal bag can dramatically improve quality of life.
Despite stigma, many patients report freedom from constant bathroom anxiety, ability to travel and socialize, and improved skin and hygiene.
It is irreversible but often life-changing for the right candidate.
Prevent Future Episodes
Prevention is the best long-term strategy. Small, consistent changes reduce recurrence.
Maintain Hydration and Fiber Balance
Drink fluids steadily throughout the day even if not thirsty. Pair adequate water with fiber to keep stools formed but soft.
Keep a Symptom and Food Diary
Track bowel movements including time, consistency, and urgency, foods eaten, medications taken, and stress levels.
Patterns often reveal hidden triggers like certain meals, medications, or stress spikes.
Schedule Regular Medication Reviews
Ask a doctor or pharmacist to review all prescriptions and supplements at least annually. Eliminate unnecessary drugs, especially proton pump inhibitors, laxatives, and nonsteroidal anti-inflammatory drugs.
Practice Bowel Training
Use the gastrocolic reflex, the natural surge in bowel activity after eating.
Sit on the toilet 20 to 30 minutes after meals. Allow time without rushing. Use proper posture with feet elevated and leaning forward.
This builds routine and improves rectal awareness.
Special Considerations for Elderly Patients
Older adults face unique challenges that require tailored care.
Watch for Atypical Symptoms
Seniors may not report classic diarrhea. Instead, look for weakness or fatigue, confusion or delirium, functional decline like not leaving the house, or increased falls.
Diarrhea can be the hidden cause.
Reduce Fall and Delirium Risk
Dehydration and nighttime urgency increase fall risk. Prevent by encouraging daytime fluid intake, limiting evening liquids, using bedside commodes, and monitoring mental status closely.
Leverage In-Home Medical Services
For frail or homebound seniors, services like DispatchHealth offer in-home IV hydration, lab testing, medication delivery, and avoidance of ER visits.
This provides timely, comfortable care without hospital stress.
Final Thoughts on Stopping Loose Bowels in the Elderly
Loose bowels in the elderly are treatable, not inevitable. By identifying causes, applying targeted home strategies, and seeking medical help when needed, most people can regain control and improve their quality of life. Start with hydration, diet, and medication review. Add pelvic floor exercises and long-term fiber support. When symptoms persist, pursue diagnosis and advanced options. With the right approach, relief is within reach.
Frequently Asked Questions About Stopping Loose Bowels in the Elderly
What causes loose bowels in elderly patients?
Loose bowels in elderly patients can be caused by infections like C. difficile, medication side effects from antibiotics or metformin, chronic conditions like irritable bowel syndrome or celiac disease, pancreatic insufficiency, and dietary intolerances. Identifying the underlying cause is essential for effective treatment.
How long should diarrhea last before seeing a doctor in elderly?
Diarrhea lasting more than 2 to 3 days in elderly patients requires medical evaluation. Older adults can deteriorate rapidly from dehydration, so prompt attention is important. Seek immediate care for fever, blood in stool, severe pain, or signs of dehydration.
What foods stop loose bowels in elderly?
Foods that help firm up stools include bananas, white rice, applesauce, toast, boiled potatoes, plain oatmeal, and lean meats. These should be followed short-term during acute episodes. Gradually increasing fiber intake after recovery supports long-term bowel health.
Can medications cause diarrhea in seniors?
Yes, many medications cause diarrhea in seniors including antibiotics, proton pump inhibitors, metformin, NSAIDs, magnesium supplements, and laxatives. A medication review with a doctor or pharmacist can identify and address offending drugs.
How do probiotics help with elderly diarrhea?
Probiotics help restore healthy gut bacteria and can shorten diarrhea duration, especially after antibiotic use. Effective strains include Lactobacillus rhamnosus GG and Saccharomyces boulardii. They are found in yogurt, kefir, and supplements.
When is fecal incontinence treatment needed in elderly?
Fecal incontinence treatment is needed when episodes disrupt daily life, cause skin breakdown, or lead to social isolation. Treatment options range from pelvic floor exercises and dietary changes to medications and advanced procedures like sacral nerve stimulation.