If you’re over 60 and waking up with shooting pain down your leg, you’re not alone. Sciatica in the elderly affects millions, often due to age-related spinal changes like spinal stenosis or degenerative disc disease. Unlike younger adults, older patients rarely experience sciatica from acute herniated discs. Instead, years of wear and tear compress the sciatic nerve, leading to radiating pain, numbness, or weakness that can turn simple activities into daily challenges.
The good news? Over 90% of elderly patients find relief within 4 to 6 weeks using conservative treatments. This guide delivers evidence-based strategies tailored specifically for older adults, focusing on safety, effectiveness, and long-term prevention so you can return to the activities you love.
Identify the Root Cause of Your Sciatica
Sciatica symptoms may look similar, but the underlying cause dictates your treatment approach. In seniors, degenerative conditions dominate, making accurate diagnosis essential for effective care.
Spinal Stenosis Is Most Common in Seniors
Narrowing of the spinal canal affects over half of adults over 60. Bone spurs, thickened ligaments, and disc collapse squeeze nerve roots, causing neurogenic claudication. This is leg pain that worsens with walking and improves when sitting or leaning forward. Many find relief by pushing a shopping cart, which is why this is called the “shopping cart sign.” Unlike disc-related sciatica, stenosis often causes bilateral leg symptoms affecting both legs.
Degenerative Disc Disease Differs From Herniated Disc
Discs lose hydration and height with age, leading to instability and nerve irritation. This is degenerative disc disease. True herniated discs are less common in the elderly because discs become stiffer and drier with age. When herniations do occur, pain is usually sharp and unilateral, worsening with sitting or bending backward.
Rule Out Spondylolisthesis
A slipped vertebra, often L4 over L5, can compress nerves and cause chronic sciatica. It may develop silently or follow trauma. Imaging is needed to confirm slippage and assess stability. Significant spondylolisthesis may require surgical evaluation.
Recognize Emergency Warning Signs Immediately
Most sciatica is manageable, but certain symptoms demand emergency care. Knowing these red flags could prevent permanent damage.
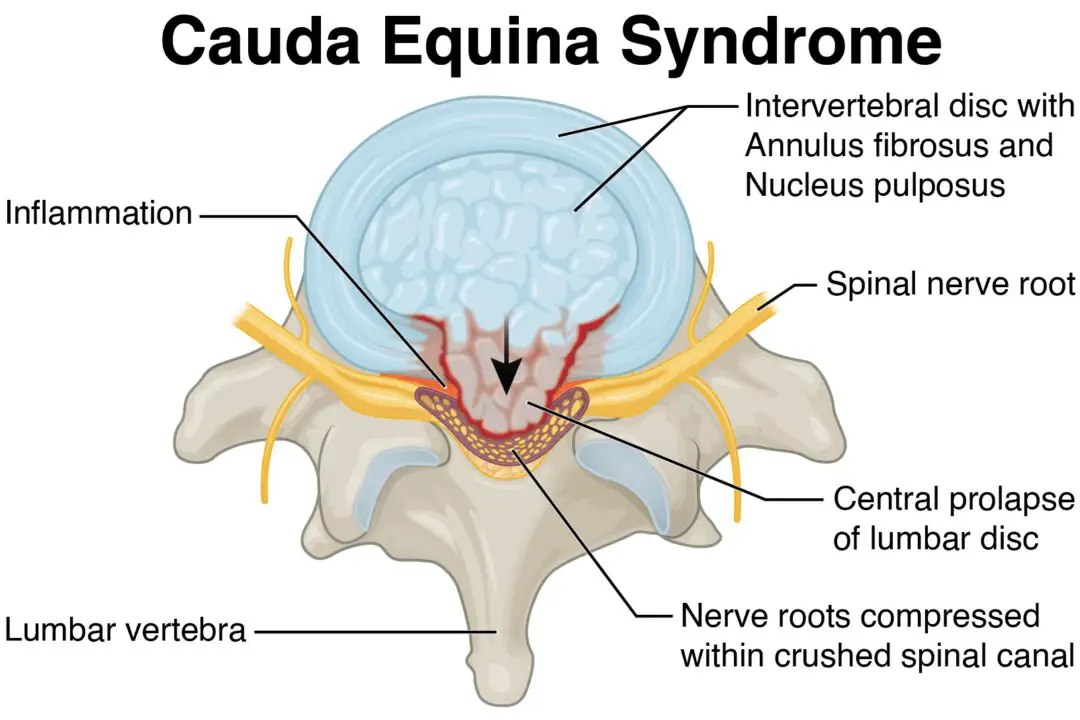
Watch for Cauda Equina Syndrome
This rare but critical condition involves severe compression of the nerve bundle at the base of the spine. Seek emergency care if you experience loss of bladder or bowel control, numbness in the groin or inner thighs known as saddle anesthesia, progressive leg weakness or foot drop, or severe unrelenting lower back and leg pain. Without prompt surgery, permanent neurological damage can occur.
When to See a Doctor Sooner
Even without red flags, consult a healthcare provider if pain lasts more than 6 weeks, you develop new numbness or weakness, walking becomes difficult, or home treatments aren’t helping. Early diagnosis prevents chronic pain and guides safe treatment specific to your condition.
Start Conservative Treatments First
Non-invasive strategies are first-line and highly effective for elderly sciatica. Most patients improve without surgery when they follow a consistent conservative plan.
Choose Pain Relievers Wisely
Medications help manage pain and inflammation, but risks increase with age. Acetaminophen is the first choice for mild to moderate pain and is safer for kidneys and stomach than NSAIDs. Monitor liver function if used regularly. NSAIDs like ibuprofen and naproxen work well for short-term inflammation but avoid them if you have kidney disease, heart failure, or GI ulcers. Use the lowest dose for the shortest duration possible.
Target Nerve Pain Directly
Neuropathic agents work best for burning, tingling, or electric shock sensations. Gabapentin or pregabalin start low and go slow, with side effects including dizziness and swelling. Duloxetine is an antidepressant that also treats nerve pain and may help with pain-related depression. Amitriptyline at low doses can improve pain and sleep but causes dry mouth and increases fall risk. Avoid long-term opioids. Tramadol or codeine may be used briefly for severe flare-ups but carry dependency and sedation risks.
Try Epidural Steroid Injections
When oral medications fail, fluoroscopically guided epidural steroid injections can reduce nerve inflammation. They offer temporary relief lasting weeks to months and allow patients to progress in physical therapy. Limit to 1 to 3 per year to minimize side effects.
Perform These 10 Safe Exercises for Sciatica Relief
Exercise is medicine for sciatica, but only if done correctly. Wrong movements can worsen degenerative conditions.
Avoid Dangerous Movements
Seniors should avoid sit-ups or crunches, deep forward bends, twisting motions like seated spinal twists, and high-impact activities like running or jumping. These increase spinal load and risk of fracture or nerve compression.
Reclined Leg Elevation
This exercise relieves pressure and improves circulation. Lie on your back with legs elevated on a chair so knees are above hip level. Add ankle pumps to boost blood flow. Hold 5 to 20 minutes multiple times daily, ideal during flare-ups.
Pelvic Tilt
This activates core muscles and stabilizes the lower back. Lie on your back with knees bent. Gently flatten your lower back by drawing your belly button toward the spine. Hold 5 to 20 seconds and repeat 10 times.
Bridge Exercise
This strengthens glutes and supports the pelvis. Lie on your back with feet flat. Lift hips to form a straight line from shoulders to knees. Hold 8 to 10 seconds, then lower slowly. Build to 2 sets of 10.
Knee Rolls
This promotes gentle spinal mobility. Lie on your back with knees bent. Gently roll knees side to side while keeping shoulders down. Perform 15 reps per side and stop if pain increases.
Single-Leg Knee Hug
This releases lumbar stiffness. Lie on your back and pull one knee to chest while keeping the other foot flat. Perform 15 reps per side.
Seated Hamstring Stretch
This reduces pull on the pelvis. Sit on a chair and extend one leg. Keep your back straight and lean forward from the hips. Hold 20 seconds and repeat 3 times per leg.
Chair Flexion
This opens space in the lower spine and is especially helpful for stenosis. Sit on a firm chair and slide hands down your legs while rounding your back. Perform 2 to 5 gentle reps several times daily.
Lumbar Flexion Forward Lean
This encourages centralization, a key sign of improvement. Sit with feet shoulder-width apart. Lean forward slowly, sliding hands down your legs. Repeat 10 times. If leg pain shifts toward the back, you’re healing.
Partial Crunch
This strengthens deep core muscles safely. Lie on your back with knees bent. Engage your core and lift shoulder blades slightly. Perform 2 sets of 15. Support your head with hands if needed.
Prone Leg Raise
This builds endurance in lower back and glutes, ideal for degenerative disc disease. Lie face down with arms folded. Tighten your abs and lift one leg a few inches. Hold 5 seconds and lower slowly. Perform 2 sets of 10.
Pro Tip: Always warm up with 2 to 3 minutes of walking in place. Perform exercises slowly and stop if pain worsens.
Apply Heat and Cold Therapy Correctly
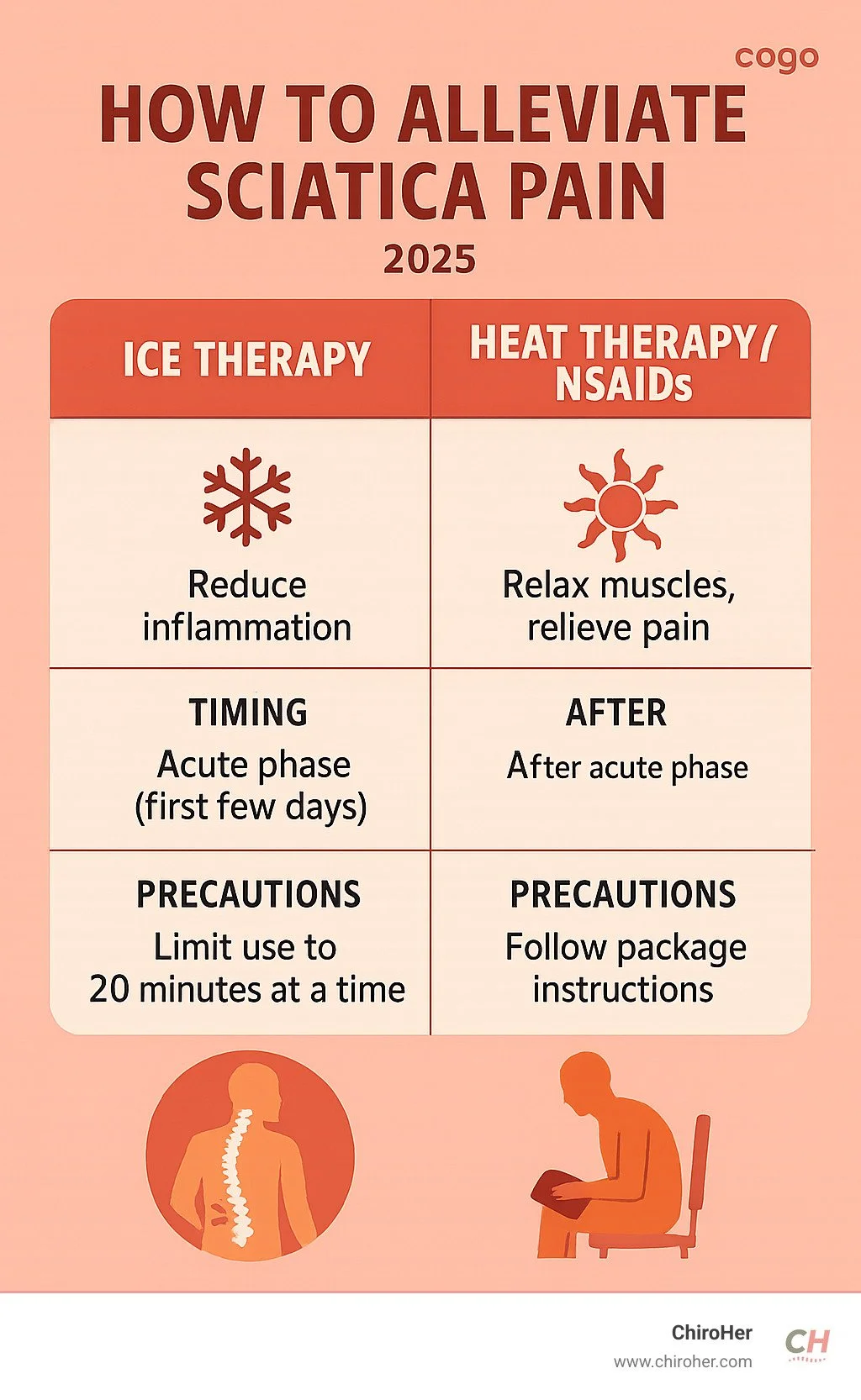
Therapy choice depends on symptom stage. Using the wrong temperature at the wrong time can worsen inflammation.
Use Cold First for Flare-Ups
Apply ice within the first 48 to 72 hours to reduce inflammation. Wrap an ice pack in a thin towel and apply for 15 to 20 minutes every 2 to 3 hours. Try ice massage using a frozen paper cup for 10 minutes, then rest for at least 1 hour. Avoid direct skin contact, especially if you have diabetes or poor circulation.
Switch to Heat After 3 Days
Heat relaxes tight muscles and boosts blood flow. Use a heating pad on low-medium setting, warm towel, or warm bath. Apply for 15 to 20 minutes 2 to 3 times daily. Always place a barrier between skin and heat source to prevent burns. Some patients benefit from alternating heat and cold, but avoid this if sensation is impaired.
Modify Daily Habits to Reduce Pain Now
Small changes yield big results in pain reduction and prevention. Your daily routines directly impact spinal health.
Stay Active, Not Stiff
Prolonged sitting or bed rest worsens sciatica. Take 5 to 10 minute walks every 2 to 3 hours. Use a cane or walker if balance is poor. Park farther away or walk around the house regularly. Movement nourishes spinal discs and reduces nerve irritation.
Lift Safely Even Light Objects
Even picking up a bag of groceries can trigger pain. Bend at the knees, not the waist. Keep the object close to your body. Avoid twisting while lifting. Limit loads to under 10 pounds.
Optimize Posture and Sleep
Use lumbar support in chairs and cars. Sit with feet flat and hips slightly above knees. Sleep on a firm mattress. Back sleepers should place a pillow under the knees. Side sleepers should place a pillow between the legs.
Lose Weight If Needed
Just 5 to 10% body weight loss reduces spinal load and inflammation. Combine gentle exercise with a balanced diet rich in anti-inflammatory foods like leafy greens, fatty fish, and nuts.
Make Your Home Safer
Install grab bars in bathrooms. Use non-slip mats in showers. Raise toilet seats and use shower benches. Avoid deep gardening by using raised beds instead.
Work With a Physical Therapist
Self-treatment can backfire. A geriatric physical therapist tailors care to your specific condition and ensures you’re doing exercises correctly.
Why Professional Guidance Matters
A physical therapist correctly identifies whether you have stenosis versus disc herniation, as treatment differs significantly. They teach safe movement patterns like how to get up from a chair properly. They provide manual therapy to improve joint mobility. They monitor for red flags during exercise.
Ron Miller, a spine specialist physical therapist with over 20 years of experience, emphasizes that elderly patients need stabilization, not stretching. Wrong exercises can make things worse. Aim for 2 to 3 sessions per week initially, then transition to a home program.
Consider Surgery Only as Last Resort
Surgery isn’t first-line but can be life-changing when appropriate and conservative measures have failed.
Know When Surgery Is Needed
Consider surgical evaluation if pain is debilitating and lasts 6 to 12 weeks, you develop progressive weakness like foot drop, you have loss of bowel or bladder control, or imaging confirms nerve compression matching your symptoms.
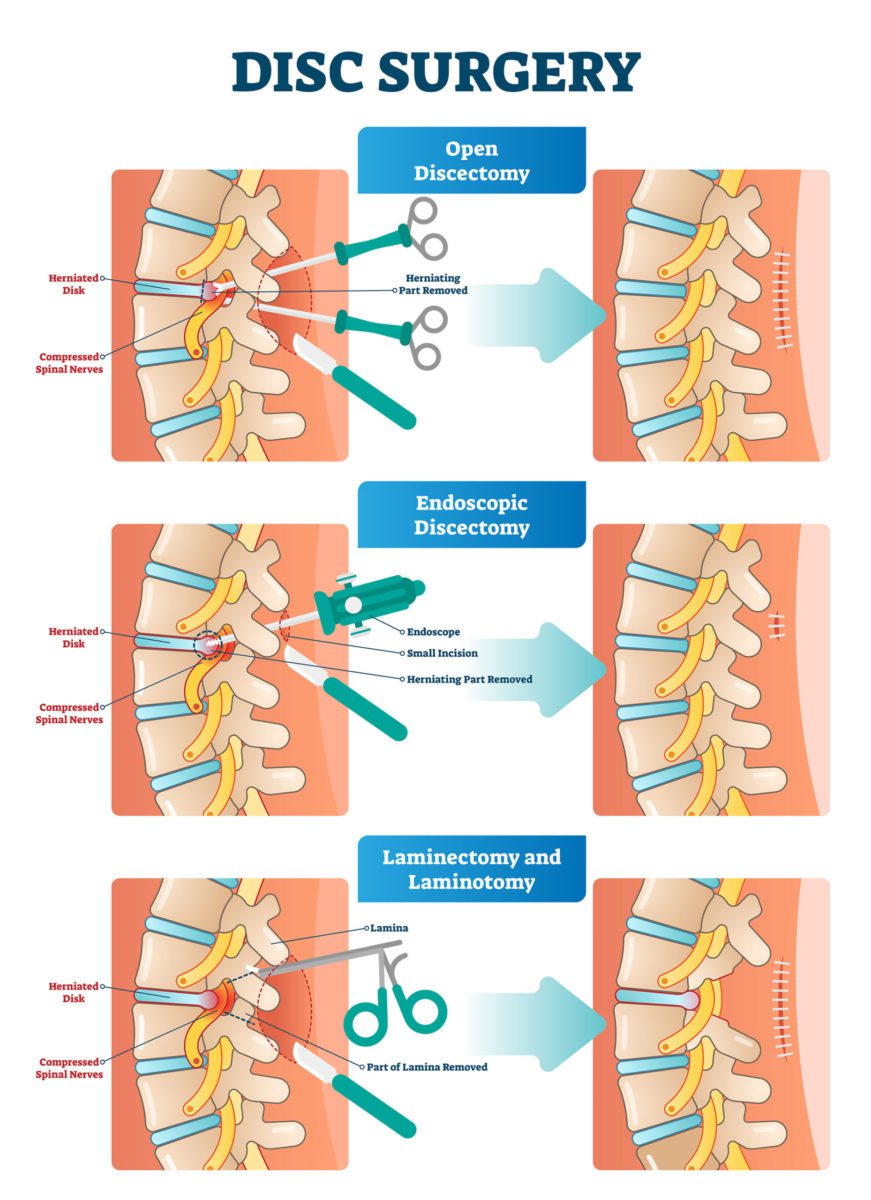
Common Procedures Explained
Microdiscectomy removes herniated disc material and works best for isolated disc herniation with leg pain. Laminectomy removes part of the vertebra to widen the spinal canal and is the gold standard for spinal stenosis. Foraminotomy enlarges the nerve exit space and is used for foraminal narrowing. Spinal fusion stabilizes slipped or unstable vertebrae and is often combined with decompression.
Risks Are Higher in Seniors
Expect longer recovery times, higher infection and blood clot risk, and potential anesthesia complications. Comorbidities like diabetes and heart disease must be optimized before surgery. A multidisciplinary team including a surgeon, geriatrician, and anesthesiologist should evaluate your fitness for surgery.
Prevent Sciatica From Returning Long-Term
Sciatica returns in up to 30% of patients, but you can reduce your risk significantly with consistent habits.
Adopt Daily Prevention Habits
Walk 20 to 30 minutes daily at a comfortable pace. Perform core stabilization exercises 3 to 4 times per week. Avoid sitting longer than 30 to 60 minutes without standing. Maintain a healthy weight and practice proper lifting mechanics.
Focus on Fall Prevention
Falls can trigger or worsen sciatica. Wear supportive non-slip shoes. Remove tripping hazards like rugs and cords. Address vision or balance issues. Try tai chi, which is proven to improve balance and reduce falls in older adults.
Support Your Mental Health During Recovery
Chronic pain affects mood and quality of life. Addressing the psychological aspect improves treatment outcomes.
Try Cognitive Behavioral Therapy
CBT helps reframe pain-related thoughts and reduce fear of movement. Studies show it improves function and reduces pain perception in older adults.
Practice Mindfulness and Breathing
Diaphragmatic breathing calms the nervous system. Guided meditation reduces pain-related stress. Progressive muscle relaxation eases tension. Just 5 to 10 minutes daily can make a difference in how you perceive pain.
Key Takeaways for Treating Sciatica in Elderly
Treating sciatica in the elderly requires a personalized, cautious approach. Focus on safe movement, professional guidance, and consistent conservative care. Over 90% of patients improve within 4 to 6 weeks without surgery. Identify whether spinal stenosis or degenerative disc disease is causing your symptoms, as treatment approaches differ. Avoid dangerous exercises like sit-ups and deep twists. Work with a geriatric physical therapist to ensure you’re doing the right movements for your condition. With the right plan, most seniors can find lasting relief and return to the activities they love.
Frequently Asked Questions About Sciatica in Elderly
How long does it take for sciatica to heal in elderly patients?
Most elderly patients experience significant improvement within 4 to 6 weeks with conservative treatment. Over 90% resolve without surgery.
Can I treat sciatica at home without seeing a doctor?
Mild cases can be managed at home with gentle exercises, heat therapy, and over-the-counter pain relievers. However, you should see a doctor if pain lasts more than 6 weeks, you develop weakness or numbness, or you experience bladder or bowel problems.
Will I need surgery for sciatica?
Surgery is typically a last resort. Most elderly patients improve with conservative treatments like physical therapy, medications, and exercise. Surgery is considered only if pain is debilitating after 6 to 12 weeks of conservative care or if you develop progressive weakness.
Is walking good for sciatica in elderly?
Yes, walking is excellent for sciatica. Take short 5 to 10 minute walks every 2 to 3 hours. Movement nourishes spinal discs and reduces nerve irritation. Avoid prolonged sitting, which worsens symptoms.
What is the best sleeping position for elderly with sciatica?
Sleep on a firm mattress. Back sleepers should place a pillow under the knees. Side sleepers should place a pillow between the legs. These positions reduce pressure on the sciatic nerve.