Hearing loss in older adults isn’t just a normal part of aging to accept, it’s a widespread, progressive condition affecting millions. Known medically as presbycusis, age-related hearing loss impacts nearly half of adults over 75 and begins much earlier than most realize. The first signs often appear subtly: struggling to follow conversations in noisy places, asking others to repeat themselves, or turning up the TV volume past a comfortable level. These aren’t just annoyances, they’re signals that the delicate auditory system is deteriorating.
The root cause lies deep within the inner ear, where tiny hair cells and nerve pathways break down over time. Unlike other cells in the body, these auditory cells do not regenerate. Once damaged, the loss is permanent. But aging isn’t the only factor. Decades of noise exposure, chronic health conditions like diabetes and hypertension, certain medications, and even genetics can accelerate the decline. This guide breaks down exactly why elderly individuals lose hearing, what happens inside the ear and brain, and how to recognize, manage, and slow the progression.
Inner Ear Degeneration Explained
The primary reason elderly individuals lose hearing is the gradual breakdown of critical structures in the inner ear, especially the cochlea and its sensory cells.
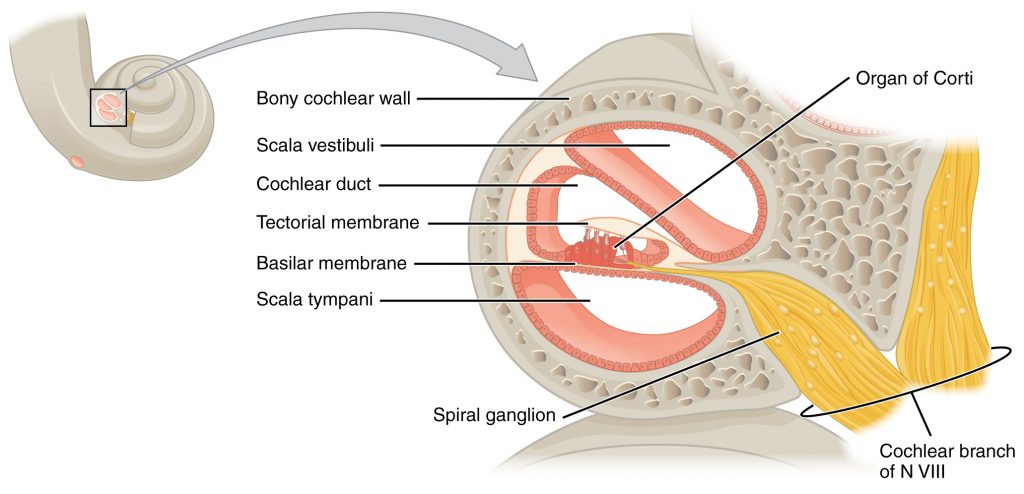
Hair Cell Damage in the Cochlea
Inside the cochlea are tiny hair cells that convert sound vibrations into electrical signals sent to the brain. With age, these cells, particularly the outer hair cells at the base of the cochlea, begin to deteriorate. This area processes high-frequency sounds, which is why seniors often lose the ability to hear children’s voices, birdsong, or consonants like s, f, and th first.
Because hair cells do not regenerate, their loss is irreversible. Over time, even low-frequency hearing may decline, making speech sound muffled or distorted.
Reduced Blood Flow to the Inner Ear
The cochlea has a high metabolic demand and relies on consistent blood flow to function. Aging often brings vascular changes, such as atherosclerosis or hypertension, that reduce circulation to the inner ear. This cochlear ischemia starves hair cells of oxygen and nutrients, speeding up their degeneration.
Conditions like diabetes and cardiovascular disease compound this risk by damaging small blood vessels, further impairing cochlear health.
Types of Age-Related Hearing Loss

Not all presbycusis is the same. The specific type determines how hearing declines and how well treatments like hearing aids work.
Sensory Presbycusis: High-Frequency Loss
This type is caused by loss of outer hair cells in the cochlea. It begins with difficulty hearing high-pitched sounds. Speech may still be understandable in quiet settings. This form is often linked to noise exposure and oxidative stress over time.
Neural Presbycusis: Poor Speech Clarity
This involves degeneration of auditory nerve fibers or brainstem pathways. It is characterized by difficulty understanding speech, even when volume is adequate. The condition worsens in noisy environments due to poor signal processing. Neural presbycusis is strongly associated with cognitive decline and reduced brain stimulation.
Diagnosing the type helps determine whether hearing aids will be effective or if more advanced options like cochlear implants are needed.
Key Causes and Risk Factors
While aging is unavoidable, several factors influence how quickly and severely hearing declines.
Biological Aging Processes
Several internal changes contribute to age-related hearing loss. Mitochondrial dysfunction reduces energy production in inner ear cells, leading to cell death. Oxidative stress accumulates free radicals that damage hair cells over decades. Genetic predisposition means family history can predict earlier onset or faster progression.
Chronic Health Conditions
Certain medical conditions significantly impact hearing health. Diabetes damages cochlear nerves and blood vessels through high blood sugar. Hypertension harms delicate inner ear circulation. Cardiovascular disease reduces blood flow, accelerating cochlear aging. Kidney disease alters fluid balance critical for inner ear function.
Lifestyle and Environmental Risks
Long-term exposure to loud sounds adds to age-related damage. Ototoxic medications like cisplatin, gentamicin, and furosemide can damage hearing, especially with long-term use. Smoking constricts blood vessels, reducing oxygen to the inner ear. Alcohol use may contribute to neurotoxic effects on auditory pathways.
Reversible Factors That Mimic Hearing Loss
Earwax buildup is common in seniors due to drier wax and reduced ear canal mobility. This condition is easily treated but often mistaken for presbycusis. Always rule out earwax blockage during evaluation.
Early Signs and Common Symptoms
Hearing loss develops slowly, so symptoms are often overlooked until they disrupt daily life.
Telltale Warning Signs
Watch for these common indicators. Frequently asking others to repeat themselves is a primary sign. Thinking people are mumbling when they speak is another clue. Needing to turn up the TV or phone volume excessively warrants attention. Missing parts of conversations, especially in groups, is concerning. Trouble hearing women’s or children’s voices indicates high-frequency loss. Misunderstanding words like cat versus bat or think versus sink is common.
Hidden but Serious Symptoms
Tinnitus, ringing or buzzing in the ears, is present in over 50% of presbycusis cases. Listening fatigue causes mental exhaustion from straining to hear. Social withdrawal occurs due to frustration or embarrassment. Cognitive strain means the brain works harder to fill in missing sounds, reducing focus on memory or comprehension.
Family members often notice these changes before the individual does.
How Hearing Loss Is Diagnosed
Early diagnosis is critical to preserving brain function and communication ability.
Physical Ear Exam
A doctor performs this exam with an otoscope to check for wax blockage, infection, or eardrum damage. This step rules out reversible causes before advanced testing.
Hearing Tests by an Audiologist
Pure-tone audiometry measures the softest sounds you can hear across frequencies. Results plotted on an audiogram show a hallmark downward slope at high frequencies for presbycusis.
Speech audiometry tests your ability to understand spoken words. It reveals speech discrimination loss, which is common in neural presbycusis.
Tympanometry assesses eardrum movement and middle ear pressure. This helps distinguish sensorineural from conductive hearing loss.
Auditory brainstem response is used in complex cases to evaluate nerve signal transmission to the brain.
Medicare covers diagnostic hearing tests when ordered by a doctor, though not hearing aids.
Effective Treatment Options
While presbycusis cannot be reversed, modern interventions restore function and connection.
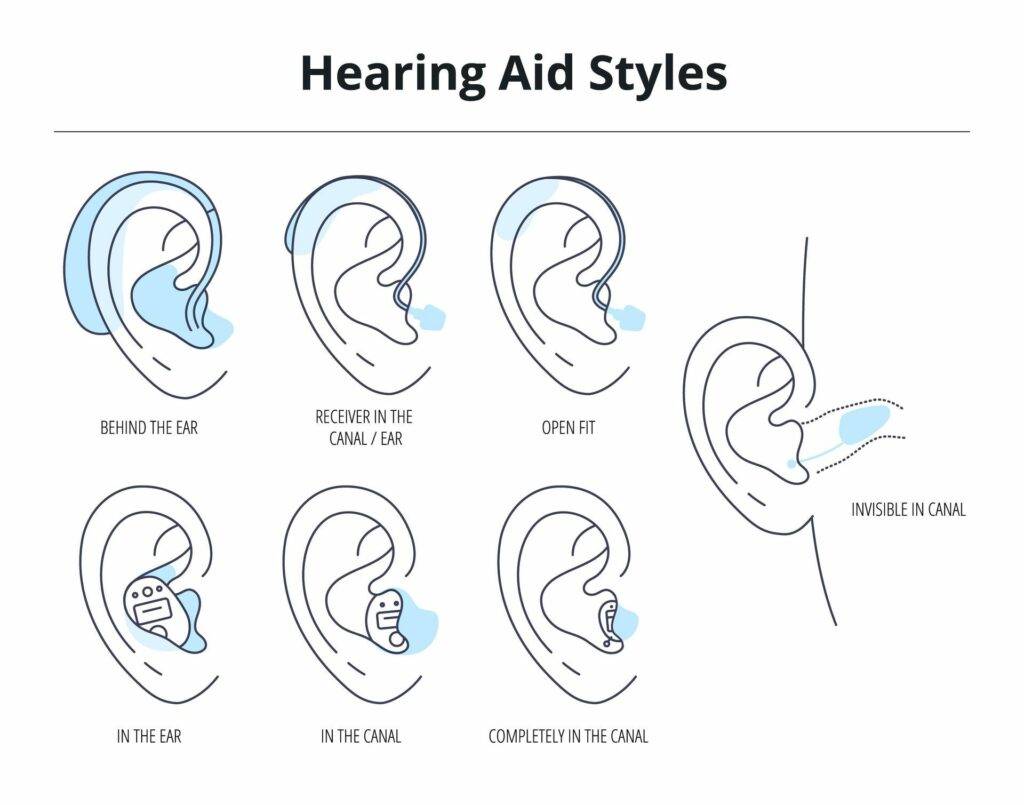
Hearing Aids: First-Line Treatment
Hearing aids amplify sounds and enhance speech clarity using digital processing. They adjust automatically to background noise thousands of times per second. Available styles include behind-the-ear, in-the-ear, and completely-in-canal. Features include Bluetooth, noise reduction, and directional microphones.
Cost and coverage vary. Traditional Medicare does not cover hearing aids. Some Medicare Advantage plans, Medicaid, or private insurance offer partial coverage. Financing plans and nonprofit assistance programs are available.
Cochlear Implants for Severe Loss
These devices are for those who get little benefit from hearing aids. They bypass damaged hair cells and stimulate the auditory nerve directly. The procedure requires surgery and auditory rehabilitation to interpret new sounds. Cochlear implants are highly effective for speech understanding in quiet and noise.
Assistive Listening Devices
TV streamers send audio directly to headphones or hearing aids. Amplified phones boost volume and clarity. Captioning apps provide real-time subtitles on calls and videos. Alerting systems use flashing lights or vibrations for doorbells, alarms, or phones.
Untreated Hearing Loss: Hidden Dangers
Ignoring hearing loss has serious consequences beyond communication.
Cognitive and Brain Health Risks
Untreated presbycusis is linked to accelerated brain atrophy and increased dementia risk. Cognitive overload occurs because the brain uses excessive resources to decode sound, reducing capacity for memory and focus. Sensory deprivation weakens neural networks over time due to lack of auditory input.
Studies show seniors with untreated hearing loss experience cognitive decline 30-40% faster than peers with normal hearing.
Emotional and Social Consequences
Depression and anxiety often result from isolation and frustration. Social withdrawal occurs due to embarrassment or effort required to communicate. Relationships with family and friends become strained.
Physical Safety Risks
Poor spatial awareness and increased cognitive load affect balance, leading to higher fall risk. Inability to hear smoke alarms, car horns, or medical alerts creates dangerous situations.
Prevention and Slowing Progression
You cannot stop aging, but you can protect your hearing.
Protect Your Ears Daily
Wear ear protection in loud environments like concerts, power tools, and lawn equipment. Follow the 60/60 rule: no more than 60% volume for 60 minutes when using headphones. Use noise-canceling headphones to avoid cranking up volume in noisy places.
Manage Chronic Conditions
Control blood pressure, blood sugar, and cholesterol. Exercise regularly to support healthy circulation. Eat a heart-healthy diet rich in antioxidants.
Avoid Ototoxic Medications
Ask your doctor about hearing risks before starting drugs like cisplatin, gentamicin, furosemide, or high-dose aspirin. Request hearing monitoring if long-term use is necessary.
Keep Ears Clean and Tested
Do not use cotton swabs, as they push wax deeper. See a professional for earwax removal if needed. Get a hearing checkup every year after age 65, even without symptoms.
Long-Term Outlook and Prognosis
Presbycusis is progressive, but the future can still be bright with intervention.
Best Prognostic Factors
Early hearing aid use preserves brain pathways and slows cognitive decline. Daily device use maximizes adaptation and benefit. Regular audiologist visits allow for tuning and monitoring.
Without Treatment
Hearing worsens, leading to functional deafness. Social isolation, depression, and dementia risk increase. Quality of life declines significantly.
With proper care, seniors can stay engaged, independent, and mentally sharp.
Frequently Asked Questions About Age-Related Hearing Loss
What is the main reason elderly people lose hearing?
The primary cause is degeneration of hair cells in the inner ear, particularly in the cochlea. These cells do not regenerate, so their loss is permanent. Additional factors include reduced blood flow, genetic predisposition, and lifetime noise exposure.
At what age does hearing loss typically begin in seniors?
Age-related hearing loss usually starts between ages 65 and 75. Approximately 30-35% of adults in this range have some hearing loss. The prevalence increases to 40-50% for those over 75 and reaches 50% for adults over 85.
Can hearing loss in the elderly be reversed?
No, the hair cell damage that causes presbycusis cannot be reversed. However, hearing aids, cochlear implants, and assistive devices can significantly improve function and quality of life. Treating reversible causes like earwax buildup can also help.
How does untreated hearing loss affect brain health?
Untreated hearing loss is linked to faster cognitive decline and increased dementia risk. The brain works harder to decode degraded sounds, leaving fewer resources for memory and thinking. Studies show cognitive decline accelerates 30-40% faster in those with untreated hearing loss.
What lifestyle factors accelerate hearing loss in older adults?
Long-term noise exposure, smoking, and ototoxic medications contribute to faster hearing decline. Chronic conditions like diabetes and hypertension also impair inner ear health. Protecting your ears and managing health conditions can slow progression.
Are hearing aids covered by Medicare?
Traditional Medicare does not cover hearing aids, though it does cover diagnostic hearing tests when ordered by a physician. Some Medicare Advantage plans, Medicaid, and private insurance may offer partial coverage. Financing plans and nonprofit programs can help with costs.
Key Takeaways for Understanding Elderly Hearing Loss
Why do elderly lose hearing? The answer lies in irreversible changes within the inner ear, accelerated by lifelong noise exposure, chronic health conditions, and natural aging processes. Hair cells in the cochlea simply cannot regenerate, making prevention critical.
Early detection matters tremendously. Scheduling a hearing evaluation at the first sign of trouble preserves brain function and communication abilities. Waiting too long allows neural pathways to weaken, making adaptation to hearing aids more difficult.
Modern treatments are highly effective. Hearing aids today are miniature computers that adjust automatically to sound environments. For severe cases, cochlear implants can restore speech understanding. Assistive devices and communication strategies further improve quality of life.
Protection is possible. Avoiding loud noises, managing blood pressure and diabetes, and monitoring ototoxic medications can slow progression. Once hearing is lost, it cannot be recovered, but you can prevent further damage.
The stakes are high. Untreated hearing loss leads to cognitive decline, depression, social isolation, and increased fall risk. Hearing is not a luxury, it is essential for safety, connection, and overall well-being in later years.